The Border Zone Between bvFTD and Primary Psychiatric Disorders - Psychiatric Times
ytemha34/AdobeStock

CATEGORY 1 CME
Premiere Date: April 20, 2023
Expiration Date: October 20, 2024
This activity offers CE credits for:
1. Physicians (CME)
2. Other
All other clinicians either will receive a CME Attendance Certificate or may choose any of the types of CE credit being offered.
ACTIVITY GOAL
The goal of this activity is to learn about frontotemporal lobar degeneration and the several overlapping syndromes that it encompasses, as well as how to distinguish behavioral variant frontotemporal lobar degeneration from other psychiatric disorders.
LEARNING OBJECTIVES
1. Understand the differential diagnosis of patients with progressive behavioral and cognitive impairment.
2. Understand the diagnosis and management of cognitive and behavioral symptoms in patients with behavioral variant frontotemporal dementia.
TARGET AUDIENCE
This accredited continuing education (CE) activity is intended for psychiatrists, psychologists, primary care physicians, physician assistants, nurse practitioners, and other health care professionals seeking to improve the care of patients with mental health disorders.
ACCREDITATION/CREDIT DESIGNATION/FINANCIAL SUPPORT
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Physicians' Education Resource®, LLC, and Psychiatric Times®. Physicians' Education Resource®, LLC, is accredited by the ACCME to provide continuing medical education for physicians.
Physicians' Education Resource, LLC, designates this enduring material for a maximum of 1.5 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
This activity is funded entirely by Physicians' Education Resource, LLC. No commercial support was received.
OFF-LABEL DISCLOSURE/DISCLAIMER
This accredited CE activity may or may not discuss investigational, unapproved, or off-label use of drugs. Participants are advised to consult prescribing information for any products discussed. The information provided in this accredited CE activity is for continuing medical education purposes only and is not meant to substitute for the independent clinical judgment of a physician relative to diagnostic or treatment options for a specific patient's medical condition. The opinions expressed in the content are solely those of the individual faculty members and do not reflect those of Physicians' Education Resource®, LLC.
FACULTY, STAFF, AND PLANNERS' DISCLOSURES AND CONFLICT OF INTEREST (COI) MITIGATION
None of the staff of Physicians' Education Resource, LLC, or Psychiatric Times or the planners of this educational activity have relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, reselling, or distributing health care products used by or on patients. Drs Abu Raya, Illanes-Manrique, and Miller note nothing to disclose regarding this article.
For content-related questions, email us at PTEditor@mmhgroup.com. For questions concerning the accreditation of this CE activity or how to claim credit, please contact info@gotoper.com and include "The Border Zone Between bvFTD and Primary Psychiatric Disorders" in the subject line.
HOW TO CLAIM CREDIT
Once you have read the article, please use the following URL to evaluate and request credit: https://education.gotoper.com/activity/ptcme23april. If you do not already have an account with Physicians' Education Resource®, LLC, you will be prompted to create one. You must have an account to evaluate and request credit for this activity.
Frontotemporal lobar degeneration (FTLD) is a clinicopathological term that encompasses a spectrum of several overlapping syndromes associated with a specific set of non–Alzheimer disease (AD) neurodegenerative histopathologies that includes the tau, TDP-43, and FET proteins. These pathological processes differently affect the frontotemporal neural networks and their subcortical connections in the thalamus, basal ganglia, and brainstem, which might explain the heterogenous clinical characteristics of FTLD spectrum disorders.1 The clinical syndromes associated with these neuropathologies involve behavior, language, and movement. However, prediction of the precise underlying pathology associated with these clinical syndromes is imperfect, and better biomarkers are needed.1,2
Frontotemporal dementia (FTD), a separate entity from FTLD, is an early-onset dementia that usually affects people younger than 65 years.2 The 3 main clinical entities subsumed under the term FTD are behavioral variant FTD (bvFTD), nonfluent variant primary progressive aphasia (nfvPPA), and semantic variant primary progressive aphasia (svPPA) (Table 1). FTD may overlap with other clinical syndromes such as amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND), progressive supranuclear palsy (PSP), or corticobasal syndrome (CBS).1
Table 1. Entities Subsumed Under Frontotemporal Dementia
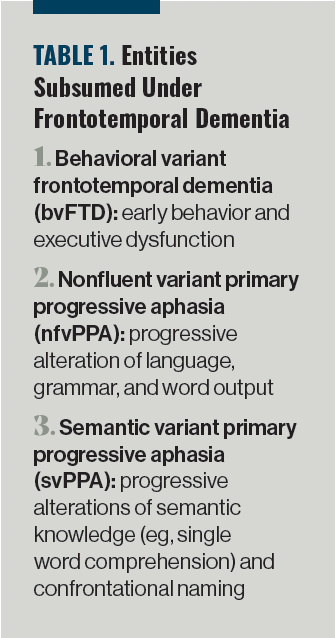
For psychiatrists, bvFTD is of particular interest because it overlaps clinically with obsessive-compulsive disorder (OCD); affective, psychotic, and personality disorders; and other psychiatric disorders. bvFTD accounts for roughly 60% of FTD cases, whereas the other 40% are language variants (nfvPPA and svPPA).2 bvFTD is the second-most common cause of dementia in adults aged less than 65 years and is probably the most common dementia for those aged younger than 60 years. The average age of onset is between 45 and 65 years, but cases have been documented in patients aged younger than 30 years and in very old patients as well.1,2
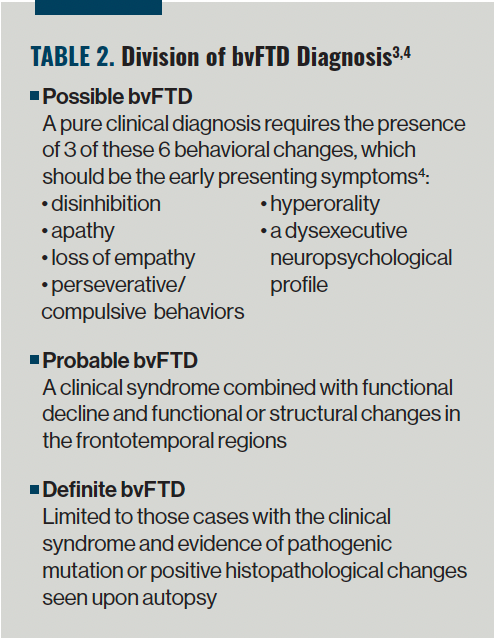
An international consortium established diagnostic criteria for bvFTD in 2011, and the diagnosis was divided into possible, probable, and definite, as outlined in Table 2.3,4 These criteria have increased the ability of clinicians to distinguish between bvFTD and other neurocognitive disorders, such as AD, but it is still difficult to distinguish bvFTD from a primary psychiatric disorder.
Table 2. Division of bvFTD Diagnosis3,4
Diagnostic Challenges
Distinguishing bvFTD from a primary psychiatric disorder can be challenging for several reasons, including the lack of definitive biomarkers, the sometimes-slow evolution of bvFTD from a primarily psychiatric condition to a dementia, and the lack of knowledge in the medical community regarding the anatomic substrates of behavior. It is estimated that about 50% of patients with FTD receive an initial misdiagnosis of depression or another psychiatric disorder.1
The sometimes-early age of symptoms onset may be a challenge for clinicians. Although bvFTD often presents in patients older than 40 years, and many primary psychiatric disorders start earlier in life, there are exceptions. Caution in this regard is necessary when a patient is diagnosed with any late-onset psychiatric disorder such as late-life depression, schizophrenia, and bipolar disorder, or OCD. In these cases, bvFTD should be considered in the differential diagnosis.
Diagnostic confusion is common when a patient meets diagnostic criteria for bvFTD but has a very slow disease course—over decades—with slow progression of cognitive impairment and often normal MRI and PET studies. This syndrome is classified as FTD phenocopy. Some patients have a primary psychiatric disturbance such as bipolar disorder, personality disorder, or autism spectrum disorder,5,6 whereas others have a slow sporadic or genetic form of bvFTD. The latter has been reported in carriers of C9orf72 pathological expansions, and these patients have had long-standing early psychiatric symptoms and late-onset psychosis that might evolve to comorbid bvFTD.7
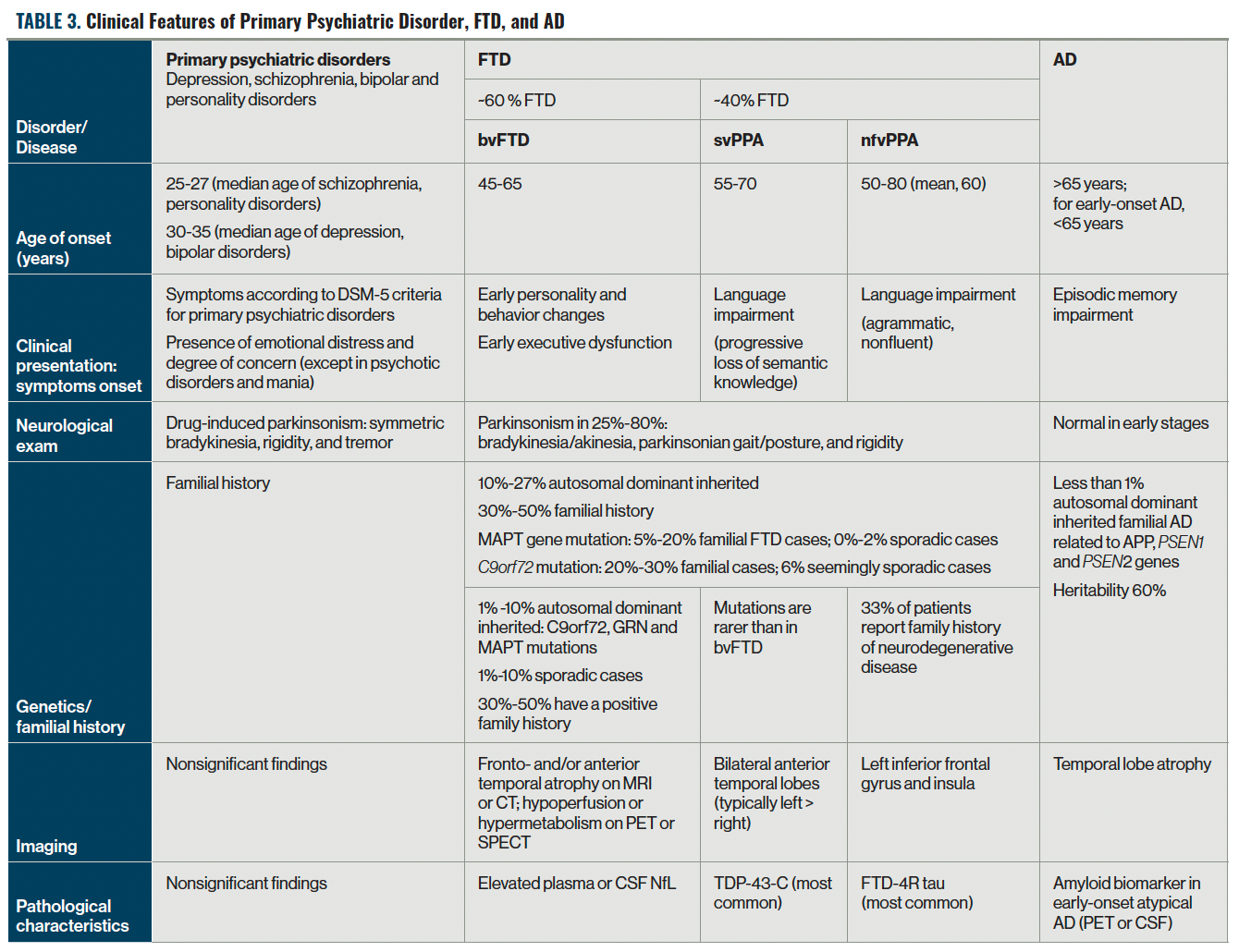
Overlapping behavioral symptoms are a major challenge in distinguishing bvFTD from a primary psychiatric disorder. For instance, bvFTD may be misdiagnosed as late-onset depression, when apathy and loss of empathy are present; as bipolar disorder, when the presentation is disinhibition; as schizophrenia or schizoaffective disorder, when psychosis is the presenting feature; and as OCD, when repetitive motor syndromes are prominent (Table 3).
Table 3. Clinical Features of Primary Psychiatric Disorder, FTD, and AD
Often, disinhibition is a presenting and core feature of bvFTD, and it is characterized by socially inappropriate behaviors and an excessive seeking of pleasurable activities that can lead to harmful social, financial, and legal consequences. Patients may present with inappropriate sexual behaviors like public masturbation or sexual harassment, touching strangers, and verbal dysdecorum with inappropriate familiarity and excessive jocularity. Theft and bad financial decisions are also common.8 When disinhibition is prominent, bvFTD is often misdiagnosed as bipolar disorder, although patients with bvFTD usually lack the expansive mood and sense of grandiosity that is seen in patients with a primary psychiatric disorder.
Apathy is also a core symptom of bvFTD and may present in a variety of ways, such as a decreased involvement in hobbies and duties, lack of spontaneous movements, decline in self-care, lack of self-awareness, and emotional flatness with impairment in personal, social, and occupational function. These changes can be misdiagnosed as manifestations of mood disorders, such as depressive disorder. When apathy is seen in bvFTD, it often presents without other typical symptoms of mood disorders such as low mood, guilt/worthlessness, or suicidal thoughts.
These diagnostic challenges contribute to the delay in the accurate diagnosis, treatment, prognosis defining and family counseling.4,9,10
Diagnostic Approach
In 2020, the Neuropsychiatric International Consortium for Frontotemporal Dementia published the first consensus recommendations to help clinicians distinguish between bvFTD and a primary psychiatric disorder. There are 8 major aspects of diagnostic evaluation of late-onset behavioral change that differentiate bvFTD from a primary psychiatric disorder.11,12
1. Patient history, including clinical scales. Clinicians should obtain a detailed history of symptoms onset, risk factors, family history, and collateral anamnesis from a knowledgeable caregiver and another independent relative or friend.
Red flags:
-Family or personal history of cognitive impairment, personality disorders, psychiatric illnesses, suicide, muscle weakness, and early sudden death
-Neurological symptoms such as tremor and other movement disorders, falls, muscle weakness, swallowing difficulties, visual difficulties, and cognitive changes
2. Psychiatric assessment. Adhere to DSM-V criteria to define the psychiatric disorders. Use a clinical scale such as the Frontal Behavioral Inventory's positive subscale and others to reduce biases during clinical assessment.
Red flags:
-Late-onset psychiatric disorder that is insidious and progressive (rather than fluctuating, waxing and waning course, or abrupt in onset, as is seen in a primary psychiatric disorder)
-Bizarre delusions and/or hallucinations are rare in bvFTD, but when present, raise suspicion for genetic forms of bvFTD such as C9orf72
-OCD with lack of insight that is not accompanied by anxiety
-Disinhibition with lack of expansive mood or sense of grandiosity or irritability13
-Apathy and mood are incongruent.
3. Physical and neurological examination findings. Consider signs of other neurodegenerative disorders such as ALS, PSP, or CBS. Consider neurological consultation in ambiguous cases.
Red flags:
-Parkinsonism, frontal release signs, pyramidal signs, weakness
4. Bedside cognitive tests and neuropsychological examination. Focus assessment on executive dysfunctions assessment, language, memory, and Frontal Assessment Battery.
Caution: Similar deficits in executive functions, verbal memory, and sensory processing might be seen in patients with bipolar disorders during manic or depressive episodes. Working memory performance can be decreased even in young patients with bipolar disorder.14
5. Tests of social cognition. Use a structured test of social cognition, such as the Ekman 60 Faces Test, to assess the degree of impairment of social cognition that occurs in bvFTD and a primary psychiatric disorder.
6. Structural and nuclear imaging. Use CT or MRI to exclude other etiologies, such as frontal brain tumors or vascular disease, and to determine the presence of brain atrophy. Symmetrical or asymmetrical atrophy in the frontal and/or temporal lobes supports diagnosis of bvFTD in the appropriate clinical setting. Functional imaging fluorodeoxyglucose PET can be used as an adjunct to structural imaging in patients with suspected bvFTD, particularly if MRI findings are normal or only questionably consistent with FTD. Amyloid PET imaging identifies individuals with amyloid deposition in the brain and can be used to differentiate underlying AD from non-AD disorders in patients with a bvFTD-like presentation.
7. Cerebrospinal fluid (CSF) and blood biomarkers. Growing evidence indicates that plasma and CSF biomarkers are sensitive and specific for AD (eg, phosphorylated tau), and these should be used to differentiate between AD and FTLD. FTLD has no specific blood or CSF biomarkers. Neurofilament light chain is a sensitive marker of neurodegeneration associated with FTD and rises to very high levels in many patients. Although high levels do not differentiate the different FTLD pathologies from one another, it may be useful in differentiating between a neurodegenerative disease and a primary psychiatric disorder in patients with a bvFTD-like presentation.15
Therefore, for at least the next few years, the role of CSF testing in a bvFTD-like presentation will be most useful in ruling out AD and in investigating the very rare infectious, autoimmune/inflammatory, and paraneoplastic processes that lead to a bvFTD syndrome.16
8. Genetic testing. Approximately 15% to 20% of FTD is genetic in etiology. Mutations in C9orf72, GRN, and MAPT genes account for nearly 50% of autosomal dominant inherited FTLD; moreover, they are associated with high prevalence (>50%) of neuropsychiatric symptoms.17 MAPT mutations present earlier in life with a mean age of onset in the sixth decade, while GRN and C9orf72 mutations typically appear in the seventh decade.18 C9orf72 mutations are strongly associated with ALS, whereas patients with GRN and MAPT mutations are predisposed to parkinsonian symptoms. Other mutations that cause FTD syndromes include TBK1, TDP-43, FUS, VCP, CHMP2B, SQSTM1, and UBQLN1. Genetic counseling is important when there is a family history of dementia and can help the patient and family weigh the pros and cons of obtaining genetic testing.12
Interventions
FTD quickly progresses to disability with limitations in daily activities and social interactions, leading to death approximately 8 years after first symptom onset. Interventions should be multidisciplinary, interprofessional, culturally sensitive, and community based. Currently, pharmacological and nonpharmacological treatments mainly address symptoms and can help manage bvFTD features. As of today, there are no approved disease-modifying drugs for the treatment of FTD.
Nonpharmacological treatments. Tailored recreational activities and behavioral support can improve neuropsychiatric and behavioral symptoms and alleviate caregiver distress. Environmental interventions should be considered; these include limiting access to money, food, pornography, or alcohol; placing locks on doors to prevent escape; and providing access to safe activities such as computer games, television, or accompanied walks. Some patients with FTD show a strong interest in the creative arts and music, which should be encouraged. In patients with FTD mutations, recent evidence suggests that greater intensity of physical and cognitive activities is associated with slower clinical decline and rate of atrophy on MRI.
The caregiver burden with FTD is profound, leading to depression, anxiety, and general health decline. Not only does this affect the caregiver, but it also diminishes the likelihood that the patient will receive proper care. In addition, the profound lack of insight in individuals with bvFTD suggest the need for increased caregiver support.1 Techniques in cognitive reappraisal and coping can change a caregiver's interpretation of the individual's behavior and can provide a sense of control for caregivers, which may reduce burden. Caregiver support should include recommendations for stress reduction like transcendental meditation, exercise, participation in caregiver support groups, respite care, and psychiatric intervention (when needed). In patients with FTD who have language impairment, speech and cognitive therapies are recommended. Attempts to combine language training with noninvasive brain stimulation, such as transcranial direct current stimulation, need more study before they can be recommended.12
Pharmacological treatments. No pharmacologic agents have been approved by the US Food and Drug Administration for managing symptoms related to bvFTD. Selective serotonin reuptake inhibitors and trazodone have the best evidence in managing behavioral changes like compulsions, agitation, aggressiveness, impulsivity, and aberrant eating.19 Selective and norepinephrine reuptake inhibitors (eg, venlafaxine) show similar patterns of efficacy and may be considered to manage apathy. Oxytocin is currently being studied for managing loss of empathy.20
Other behavioral abnormalities or psychotic features can be managed with low doses of atypical antipsychotics, mainly quetiapine and risperidone.21 These antipsychotic treatments should be prescribed cautiously for elderly people regardless of their comorbidities, because of the heightened risk of mortality secondary to cardio-cerebrovascular disease, falls, and infections.22
Although cholinesterase inhibitors show a positive effect on behavioral symptoms in AD, they are not beneficial and can even worsen behavioral abnormalities in patients with FTD.23 Memantine does not improve or delay progression of FTD symptoms and may even have deleterious adverse effects.
Advances in the diagnostics of FTD and the underlying pathobiologies will lead to new potential therapeutic targets for the development of effective disease-modifying drugs. For instance, the discovery of the pathogenic expansion in C9orf72 as the most common cause of inherited FTD has increased interest in the development of antisense oligonucleotides to reduce concentrations of potentially toxic mRNAs.24
Case Example
"Mr Roman," a 48-year-old man, presented to the psychiatric emergency department (ED) for bizarre behavior, claiming he had been persecuted by FBI agents because of files he kept for himself that endangered the country. He suspected the agents were spying on him and sending women to tempt him. Mr Roman was aggressive at night and was referred to the ED while trying to escape from his home. He was examined in the ED by a physician and a neurologist, and the latter decided to perform a full workup due to subfebrile fever and mild leukocytosis. The workup to rule out encephalitis, including blood tests and a lumbar puncture, was normal. His brain CT was interpreted as normal. Results of autoimmune, paraneoplastic, and toxic panels were all negative.
The attending psychiatrist obtained more extensive collateral information from Mr Roman's wife. She reported living with him for the past 10 years. After their marriage, she reported that he preferred to be by himself, did not have close friends, and avoided large gatherings. He became more socially withdrawn and unempathic, rigid, and "emotionally flat," making it "hard to get a reaction out of him." She reported that he had been employed as an attorney but had lost his job 2 years earlier. His employer had described him as disorganized, struggling with articulation in court and sometimes seeming to "lose his train of ideas." In the past year, he could not manage his finances and accumulated significant credit card debt. In the few months before evaluation, he started to become difficult to manage at home. He spent many hours every day and during the night compulsively closing windows and doors. He could not sleep well. He lost interest in his hobbies and sex. He spent increasing amounts of time "staring" at the television.
Past medical history was unrevealing, with no alcohol or drug abuse. Family history was negative for neurodegenerative diseases. A nephew had autism. His mother, who died by suicide in her 40s, had a history of depression.
Three months later, Mr Roman came for a follow-up visit to manage his antipsychotic treatment. He and his wife both reported improvement after starting the medication; however, she believed that he was becoming more apathetic, demotivated, inattentive, and disorganized, and, additionally, that his gait had started to deteriorate.
He was fully oriented, had a flat affect, and hypomimia. He was fluent with preserved naming, repetition, and comprehension. Cranial nerves were intact, including normal saccades. He had mild hyperrigidity in all 4 limbs. Sensory and motor examinations were normal. The snout reflex was negative, whereas grasp reflexes and palmomental reflexes were positive.
On cognitive testing, he scored 27 of 30 on the Mini-Mental State Examination and 15 of 30 on the Montreal Cognitive Assessment, losing points for attention, concentration, working memory items, and the Trail-Making B test sample. Semantic and phonemic fluency were both moderately impaired. The Complex Benson Figure copy and recall were normal.
A year later, Mr Roman was referred to a neurologist for complaints about muscle cramps and difficulties swallowing and climbing stairs. His neurologist found symptoms of muscle atrophy in his hands, including intrinsic muscles, bilateral grip weakness, and proximal muscle weakness, including a head drop. His jaw jerk was noticeable and exhibited pyramidal signs. He completed an EMG test that revealed activity that suits MND. Based on these findings, the diagnosis of FTD-ALS was considered.
Mr Roman was offered palliative care and he accepted. Advanced directives were signed, which requested comfort care only. He was taken off the antipsychotic because of the concern that it would exacerbate swallowing difficulty. Mr Roman had no negative consequences from the medication withdrawal. Swallowing difficulty for liquids was improved by adding thickeners. Within 3 months, Mr Roman was unable to leave his bed. By 4 months, he was unable to take in food or liquids, and died comfortably at his home with loved ones at the bedside.
Concluding Thoughts
FTD is a common early-onset dementia, with bvFTD constituting the most common type. Because bvFTD is characterized by predominant behavioral presenting symptoms that usually overlap with those of other psychiatric disorders, distinguishing the initial changes of this devastating neurodegenerative disease from common psychiatric disorders is essential for management and life-planning considerations.
Once diagnosis is made, a multidisciplinary management approach is needed. Unclear or atypical cases with behavioral symptoms or atypical psychiatric presentation may need a broader assessment regimen that includes neuropsychological and neurological examinations, tests of social cognition, neuroimaging, blood and cerebrospinal fluid tests, and genetic testing.
A wide interprofessional collaboration between neurologists and psychiatrists is needed to advance better understanding of bvFTD and to upgrade the diagnostic and management guidelines. This will be crucial as the field moves toward disease prevention, early identification, and finding personalized disease-modifying treatments.
Dr Abu Raya is a neurologist in the cognition and stroke unit at Rambam Medical Center, Haifa, Israel, and an Atlantic Fellow at the Global Brain Health Institute. Dr Illanes-Manrique is a psychiatrist and chief of the Neurogenetics Research Center at the Instituto Nacional de Ciencias Neurologicas, Lima, Peru, and an Atlantic Fellow at the Global Brain Health Institute. Dr Miller holds the A.W. and Mary Margaret Clausen Distinguished Professorship in Neurology at the University of California, San Francisco, directs the UCSF Memory and Aging Center, and is the founding director of the Global Brain Health Institute at UCSF.
Acknowledgments: The authors thank Caroline Prioleau, University of California, San Francisco, for her assistance and reviewing the manuscript.
References
1. Boeve BF. Behavioral variant frontotemporal dementia. Continuum (Minneap Minn). 2022;28(3):702-725.
2. Onyike CU, Diehl-Schmid J. The epidemiology of frontotemporal dementia. Int Rev Psychiatry. 2013;25(2):130-137.
3. Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain. 2011;134(Pt 9):2456-2477.
4. Ahmed RM, Hodges JR, Piguet O. Behavioural variant frontotemporal dementia: recent advances in the diagnosis and understanding of the disorder. Adv Exp Med Biol. 2021;1281:1-15.
5. Davies RR, Kipps CM, Mitchell J, et al. Progression in frontotemporal dementia: identifying a benign behavioral variant by magnetic resonance imaging. Arch Neurol. 2006;63(11):1627-1631.
6. Kipps CM, Hodges JR, Hornberger M. Nonprogressive behavioural frontotemporal dementia: recent developments and clinical implications of the 'bvFTD phenocopy syndrome.' Curr Opin Neurol. 2010;23(6):628-632.
7. Khan BK, Yokoyama JS, Takada LT, et al. Atypical, slowly progressive behavioural variant frontotemporal dementia associated with C9ORF72 hexanucleotide expansion. J Neurol Neurosurg Psychiatry. 2012;83(4):358-364.
8. Liljegren M, Naasan G, Temlett J, et al. Criminal behavior in frontotemporal dementia and Alzheimer disease. JAMA Neurol. 2015;72(3):295-300.
9. Peet BT, Castro-Suarez S, Miller BL. The neuropsychiatric features of behavioral variant frontotemporal dementia. Adv Exp Med Biol. 2021;1281:17-31.
10. Younes K, Miller BL. Neuropsychiatric aspects of frontotemporal dementia. Psychiatr Clin North Am. 2020;43(2):345-360.
11. Ducharme S, Dols A, Laforce R, et al. Recommendations to distinguish behavioural variant frontotemporal dementia from psychiatric disorders. Brain. 2020;143(6):1632-1650.
12. Pressman PS, Matlock D, Ducharme S. Distinguishing behavioral variant frontotemporal dementia from primary psychiatric disorders: a review of recently published consensus recommendations from the Neuropsychiatric International Consortium for Frontotemporal Dementia. J Neuropsychiatry Clin Neurosci. 2021;33(2):152-156.
13. Ducharme S, Price BH, Larvie M, et al. Clinical approach to the differential diagnosis between behavioral variant frontotemporal dementia and primary psychiatric disorders. Am J Psychiatry. 2015;172(9):827-837.
14. Maia da Silva MN, de Gobbi Porto FH, Gomes Lopes PM, et al. Frontotemporal dementia and late-onset bipolar disorder: the many directions of a busy road. Front Psychiatry. 2021;12:768722.
15. Eratne D, Loi SM, Walia N, et al. A pilot study of the utility of cerebrospinal fluid neurofilament light chain in differentiating neurodegenerative from psychiatric disorders: a 'C-reactive protein' for psychiatrists and neurologists? Aust N Z J Psychiatry. 2020;54(1):57-67.
16. Illán-Gala I, Lleo A, Karydas A, et al. Plasma Tau and neurofilament light in frontotemporal lobar degeneration and Alzheimer disease. Neurology. 2021;96(5):e671-e683.
17. Peet BT, Spina S, Mundada N, La Joie R. Neuroimaging in frontotemporal dementia: heterogeneity and relationships with underlying neuropathology. Neurotherapeutics. 2021;18(2):728-752.
18. Solmi M, Radua J, Olivola M, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022;27(1):281-295.
19. Mitchell E, Tavares TP, Palaniyappan L, Finger EC. Hoarding and obsessive–compulsive behaviours in frontotemporal dementia: clinical and neuroanatomic associations. Cortex. 2019;121:443-453.
20. Finger EC, MacKinley J, Blair M, et al. Oxytocin for frontotemporal dementia: a randomized dose-finding study of safety and tolerability. Neurology. 2015;84(2):174-181.
21. Moheb N, Charuworn K, Ashla MM, et al. Repetitive behaviors in frontotemporal dementia: compulsions or impulsions? J Neuropsychiatry Clin Neurosci. 2019;31(2):132-136.
22. Bozeat S, Gregory CA, Ralph MA, Hodges JR. Which neuropsychiatric and behavioural features distinguish frontal and temporal variants of frontotemporal dementia from Alzheimer's disease? J Neurol Neurosurg Psychiatry. 2000;69(2):178-186.
23. Perry DC, Whitwell JL, Boeve BF, et al. Voxel-based morphometry in patients with obsessive-compulsive behaviors in behavioral variant frontotemporal dementia. Eur J Neurol. 2012;19(6):911-917.
24. Bang J, Spina S, Miller BL. Frontotemporal dementia. Lancet. 2015;386(10004):1672-1682.

Comments
Post a Comment